ARTICLE SUMMARY:
Intact Vascular’s bet on a small implant to treat post-angioplasty dissections in peripheral arteries appears to be paying off.
The chief endovascular tool used to restore blood flow to diseased peripheral arteries—the angioplasty balloon—is designed to stretch the artery and break apart the occlusion-causing plaque, that is, controlled dissection of the occlusion is one of the mechanisms by which revascularization technologies work. However, in many cases, interventions leave behind dissections in the endothelium of the artery, and that’s not a good thing. Removing plaque by atherectomy can also result in arterial dissections.
These tears in the lining of the arterial wall set up an inflammatory healing response that encourages vessel occlusion. Sometimes dissections are pockets behind which blood can pool and clot, or they’re flaps of torn tissue hanging into the lumen of the artery, where they perturb blood flow and cause the artery to narrow.
Unfortunately, arterial dissections are not an infrequent complication of balloon angioplasty and atherectomy; according to one study, in the SFA (superficial femoral artery) they happen in about 84% of cases, and 42% of the time, they’re serious).
Other studies have found that even mild dissections, when associated with longer lesions, are troublesome, as are dissections with a large circumference. Finally, it’s likely that the prevalence of post-procedure dissections is even higher than is suggested by the evidence that’s been gathered so far, since, while they can be clearly seen on intravascular ultrasound, they often remain hidden in angiographic views, the most common form of imaging during interventional cardiology and vascular procedures.
Until Intact Vascular Inc. came along, stents were the solution for treating dissections, but as noted, when it comes to peripheral artery disease, they’ve come under scrutiny. “With stenting, you get total coverage of the lesion end to end, and that might sound like a good idea, but there are long term implications,” says the company’s President and CEO Bruce Shook.
“First, there is in-stent restenosis. Second, you are basically lining the entire artery with metal, which limits your ability to do things with that lesion down the road. It also limits the ability of the artery to flex normally, and in a flexing area of the leg, there is the risk that the stent might fracture,” he says.
After a peripheral angioplasty procedure, clinicians will always check to see if they’ve created any dissections in the process. If they have, they have to weigh their options against the uncertainty of whether a dissection is going to cause a problem or not, based on its circumference, the length of the lesion, the co-morbidities of the patient, and other clinical factors that haven’t been codified to create any kind of standard of care here.
Their conundrum: leave it alone and hope that everything will be fine, or stent it, with full knowledge of the complications of stents, possibly precluding future treatment options in patients who are highly likely to need them. Because in-stent restenosis is challenging to treat, many will think twice before putting in a stent. “When the entire length of a stent re-occludes, in many cases it’s challenging to reopen it, and once you have, then what are you going to do? There is already a stent in the artery,” says Shook. “We think we solve that with a minimal metal approach.”
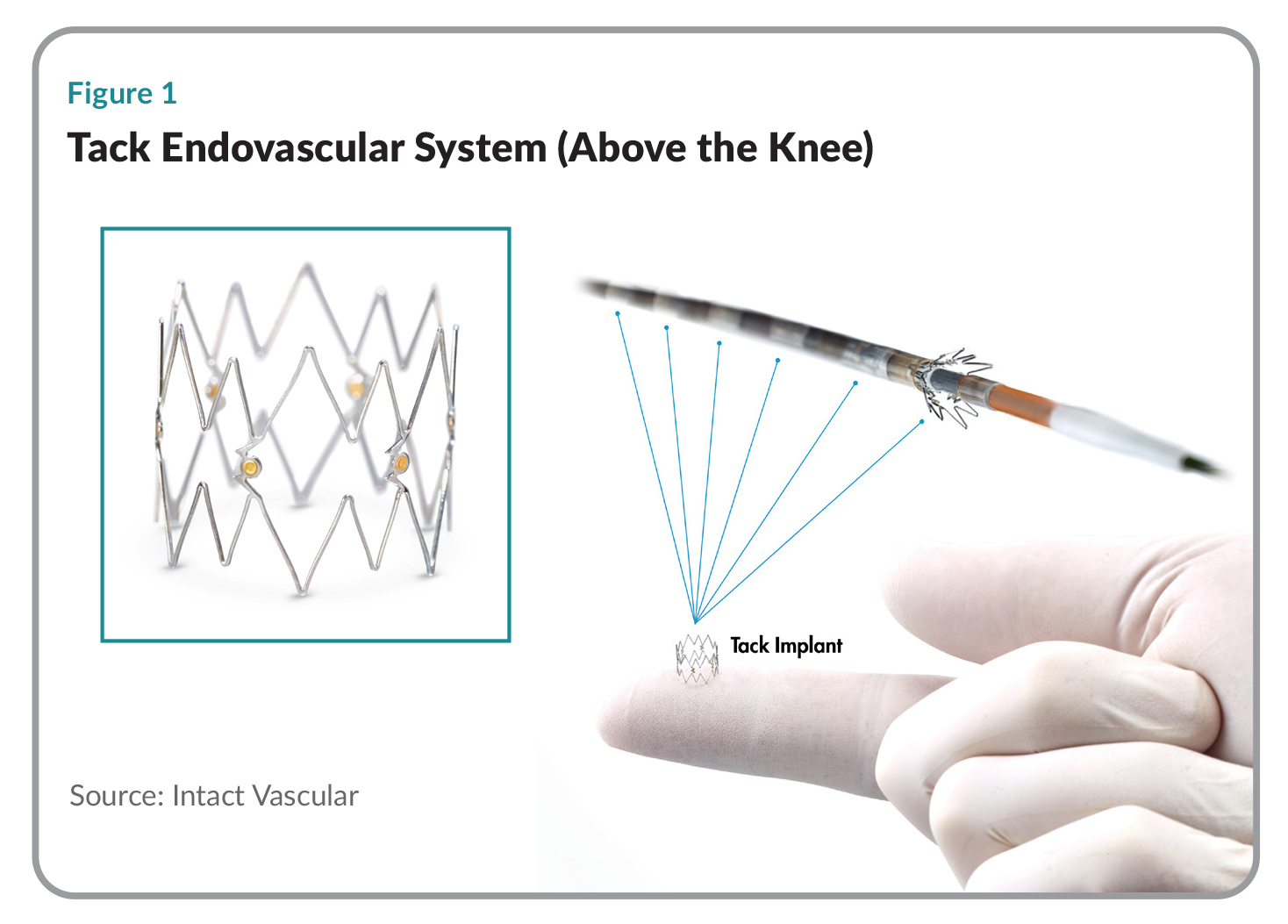 Intact Vascular’s Tack Endovascular System consists of an over-the-wire delivery system that comes preloaded with six (for above the knee applications) or four (below the knee) self-expanding nitinol implants, each 6mm in length when deployed. These pre-loaded implants can be individually deployed to treat multiple locations with a single catheter. Tack has gold radiopaque markers to make them easy to see under fluoroscopy, and anchors designed to keep them in place (see Figure 1).
Intact Vascular’s Tack Endovascular System consists of an over-the-wire delivery system that comes preloaded with six (for above the knee applications) or four (below the knee) self-expanding nitinol implants, each 6mm in length when deployed. These pre-loaded implants can be individually deployed to treat multiple locations with a single catheter. Tack has gold radiopaque markers to make them easy to see under fluoroscopy, and anchors designed to keep them in place (see Figure 1).
In the cath lab, interventionalists will run a guidewire down the diseased artery, where they can see in real time the stenosis that is occluding blood flow. First they pass an angioplasty balloon (drug coated or plain) down the guidewire and inflate it to open up the artery, after which they deflate the balloon, pull it out, and inject contrast agent into the artery to see the result—whether they’ve succeeded in opening the lesion or created any dissections. If a dissection is deemed serious enough to repair, they will advance the Tack delivery system over the same guidewire and drop in Tack implants wherever they see dissections. That can happen in multiple spots along the entire dilated length of the lesion.
As compared to a stent, treatment of a dissection using Tack leaves roughly 70-80% less metal behind. “Tacks are very small—just 6mm long—and the average patient gets four so you’re talking about 24mm of implant versus what might be 200mm of stent,” Shook says. Tack is thus likely to be much less inflammatory than a stent, and, says Shook, “You keep your future treatment options open. Most of the artery is untouched; it doesn’t have metal in it. So if you need to come back later and do a vascular anastomosis for a bypass graft, you have plenty of real estate to work with.” If the disease progresses over the years, and it usually does, a clinician can still stent the artery.
Shook describes Intact Vascular’s market as one million angioplasties in the leg each year, a patient population that breaks down into two groups of disease; above-the-knee and below-the-knee. The former is the largest market in terms of procedure volumes, but in the latter, the Tack Endovascular System shines particularly brightly because it can change the lives of very sick patients with critical limb ischemia who have a very poor prognosis if blood flow to their lower limb is not restored. Patients with CLI face amputation rates as high as 40% at six months, and mortality rates of 20% to 25% within a year of diagnosis.
At the recent VIVA meeting, six months results were presented on TOBA II BTK, Intact’s prospective, single arm clinical study for patients with CLI due to arterial disease below-the knee.
At six months, the Tack implants resolved 100% of the dissections, and 73.8% of leg wounds healed or improved. Most of the patients (95.7%) experienced amputation-free survival, 87.3% exhibited target lesion patency and a significant improvement in the toe brachial index (a measure of blood flow to the toes). The majority (92%) did not need a clinically driven intervention.
 Trial MyStrategist.com and unlock 7-days of exclusive subscriber-only access to the medical device industry's most trusted strategic publications: MedTech Strategist & Market Pathways. For more information on our demographics and current readership click here.
Trial MyStrategist.com and unlock 7-days of exclusive subscriber-only access to the medical device industry's most trusted strategic publications: MedTech Strategist & Market Pathways. For more information on our demographics and current readership click here.