
ARTICLE SUMMARY:
At the VIVA meeting in early November, Intact Vascular unveiled unprecedented clinical data for a first-of-its-kind product. Its contrarian bet on a small implant for the treatment of post-angioplasty dissections in peripheral arteries appears to be paying off.
The story of Intact Vascular Inc. begins at Christmas. Vascular surgeon Peter Schneider, MD, who currently works at the University of California at San Francisco, was stapling strings of lights onto his house, a tricky task that involves precisely placing the staples so you don’t staple through the electric wire. He mused, “Could I do what I’m doing here inside an artery?”
Meaning, would it be possible to selectively and focally repair dissections in the lumen of an artery without laying down several centimeters of metal in the form of a stent?
That “Aha moment” inspired Schneider to develop some prototypes, then, with engineer Robert Giasolli, (who is now CTO of peripheral artery disease companyCagent Vascular) to create an early version of a tiny implant that could be placed along an artery to repair the vessel dissections that are fairly common after interventional treatments for peripheral artery disease (PAD). They and Carol Burns (now Cagent Vascular’s president and CEO) founded Intact Vascular in 2011 to develop the Tack Endovascular System. In 2012, Intact Vascular raised a $15.5 million Series A round, co-led by Quaker Partners and H.I.G. BioVentures with the participation of angel investors.
At the time, with its minimalist approach, Intact was swimming against the tide; stents were a popular solution for treating occluded peripheral arteries in the legs and repairing dissections. “The full metal jacket approach was very much in fashion,” says Bruce Shook, Intact Vascular’s President and CEO. Indeed, one interventional cardiologist, who is a high volume user of Tack today, said that when he first saw it a few years ago, he didn’t know where it would fit into his practice. “It looks like a stent without much radial force. Why wouldn’t I prefer a stent?” he said. And as a small start-up with a novel idea, Intact would be going up against large companies with broad portfolios for peripheral artery disease.
Intact Vascular persevered, raising $88 million over the next eight years, and in that time, the market moved toward the company. Over time it became apparent that stents in the legs are subject to high rates of restenosis, and as PAD patients often ended up needing subsequent reinterventions, metal lined arteries became obstacles to future bypass procedures and other interventions.
Today, the trend is toward vessel-preserving interventions like atherectomy and drug coated balloon (DCB) angioplasty and leaving very little metal behind. In that paradigm, Intact Vascular fills a large unmet clinical need with Tack. “The pendulum has really swung in that direction over the ensuing years,” says Shook. “Today, we all understand that minimizing foreign material in the artery is the best approach in the long run.”
Intact Vascular has FDA approval to treat dissections above the knee and it’s on track to be the first company ever to deliver an implant that can treat post-angioplasty dissections in arteries below the knee.
Intact Vascular offers an alternative to stenting, one that permits focal treatment with minimal metal, treating the areas where there are dissections, and leaving healthy tissue alone. It thus doesn’t over-treat by covering healthy tissue, as stents do, undertreat, or exert too much radial force for the job. In essence, the Tack system allows operators to repair the damage they can see immediately after angioplasty without the downsides that have long been associated with stenting.
Intact Vascular has FDA approval to treat dissections above the knee and it’s on track to be the first company ever to deliver an implant that can treat post-angioplasty dissections in arteries below the knee (BTK), helping many seriously ill patients who otherwise might progress to gangrene and amputation.
At the recent annual meeting of VIVA [Vascular Interventional Advances], which took place in Las Vegas in early November, George Adams, MD, co-principal investigator of the company’s TOBA II BTK study, presented sterling six month data demonstrating that Tack, when used with a drug coated balloon, has a positive impact on patients with critical limb ischemia (CLI), people who face a high near-term risk of limb amputation and death. “This is the first time anyone has run a pivotal trial for below-the-knee disease and succeeded,” says Shook. Peter Schneider appears to have been right.
The Problem of Dissections
The chief endovascular tool used to restore blood flow to diseased peripheral arteries—the angioplasty balloon—is designed to stretch the artery and break apart the occlusion-causing plaque, that is, controlled dissection of the occlusion is one of the mechanisms by which revascularization technologies work. However, in many cases, interventions leave behind dissections in the endothelium of the artery, and that’s not a good thing. Removing plaque by atherectomy can also result in arterial dissections.
These tears in the lining of the arterial wall set up an inflammatory healing response that encourages vessel occlusion. Sometimes dissections are pockets behind which blood can pool and clot, or they’re flaps of torn tissue hanging into the lumen of the artery, where they perturb blood flow and cause the artery to narrow. Arterial segments that experience dissections result in target lesion revascularization rates that are more than three times higher (10.5% vs 37%) than lesions without dissections (according to an article in the August 2019 issue of the Journal of Vascular Disease Management, by Gabriel T. Brandner, et al).
Unfortunately, arterial dissections are not an infrequent complication of balloon angioplasty and atherectomy; according to one study, in the SFA (superficial femoral artery) they happen in about 84% of cases, and 42% of the time, they’re serious (see the article by M. Fujihara et al, in the June 2017 issue of the Journal of Endovascular Therapy).
Other studies have found that even mild dissections, when associated with longer lesions, are troublesome, as are dissections with a large circumference. Finally, it’s likely that the prevalence of post-procedure dissections is even higher than is suggested by the evidence that’s been gathered so far, since, while they can be clearly seen on intravascular ultrasound, they often remain hidden in angiographic views, the most common form of imaging during interventional cardiology and vascular procedures.
Minimizing Metal
Until Intact Vascular came along, stents were the solution for treating dissections, but as noted, when it comes to peripheral artery disease, they’ve come under scrutiny. “With stenting, you get total coverage of the lesion end to end, and that might sound like a good idea, but there are long term implications,” says Shook.
“First, there is in-stent restenosis. Second, you are basically lining the entire artery with metal, which limits your ability to do things with that lesion down the road. It also limits the ability of the artery to flex normally, and in a flexing area of the leg, there is the risk that the stent might fracture,” he says.
After a peripheral angioplasty procedure, clinicians will always check to see if they’ve created any dissections in the process. If they have, they have to weigh their options against the uncertainty of whether a dissection is going to cause a problem or not, based on its circumference, the length of the lesion, the co-morbidities of the patient, and other clinical factors that haven’t been codified to create any kind of standard of care here.
 Their conundrum: leave it alone and hope that everything will be fine, or stent it, with full knowledge of the complications of stents, possibly precluding future treatment options in patients who are highly likely to need them. Because in-stent restenosis is challenging to treat, many will think twice before putting in a stent. “When the entire length of a stent re-occludes, in many cases it’s challenging to reopen it, and once you have, then what are you going to do? There is already a stent in the artery,” says Shook. “We think we solve that with a minimal metal approach.”
Their conundrum: leave it alone and hope that everything will be fine, or stent it, with full knowledge of the complications of stents, possibly precluding future treatment options in patients who are highly likely to need them. Because in-stent restenosis is challenging to treat, many will think twice before putting in a stent. “When the entire length of a stent re-occludes, in many cases it’s challenging to reopen it, and once you have, then what are you going to do? There is already a stent in the artery,” says Shook. “We think we solve that with a minimal metal approach.”
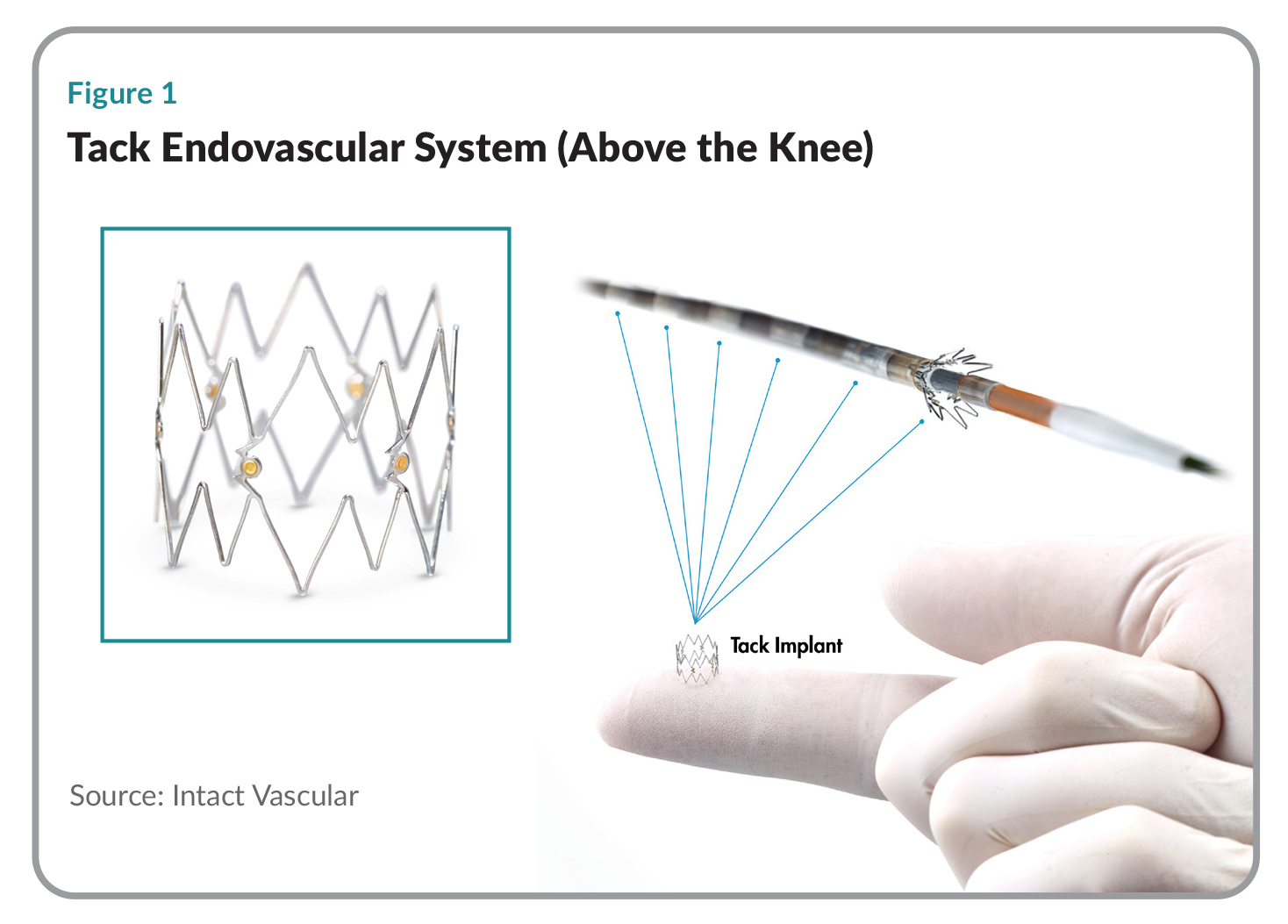
The Tack Endovascular System consists of an over-the-wire delivery system that comes preloaded with six (for above the knee applications) or four (below the knee) self-expanding nitinol implants, each 6mm in length when deployed. These pre-loaded implants can be individually deployed to treat multiple locations with a single catheter. Tack has gold radiopaque markers to make them easy to see under fluoroscopy, and anchors designed to keep them in place (see Figure 1).
In the cath lab, interventionalists will run a guidewire down the diseased artery, where they can see in real time the stenosis that is occluding blood flow. First they pass an angioplasty balloon (drug coated or plain) down the guidewire and inflate it to open up the artery, after which they deflate the balloon, pull it out, and inject contrast agent into the artery to see the result—whether they’ve succeeded in opening the lesion or created any dissections. If a dissection is deemed serious enough to repair, they will advanced the Tack delivery system over the same guidewire and drop in Tack implants wherever they see dissections. That can happen in multiple spots along the entire dilated length of the lesion.
As compared to a stent, treatment of a dissection using Tack leaves roughly 70-80% less metal behind. “Tacks are very small—just 6mm long—and the average patient gets four so you’re talking about 24mm of implant versus what might be 200mm of stent,” Shook says. Tack is thus likely to be much less inflammatory than a stent, and, says Shook, “You keep your future treatment options open. Most of the artery is untouched; it doesn’t have metal in it. So if you need to come back later and do a vascular anastomosis for a bypass graft, you have plenty of real estate to work with.” If the disease progresses over the years, and it usually does, a clinician can still stent the artery.
Turning Point
When Bruce Shook joined as CEO in 2014, Intact Vascular had generated some preliminary clinical data—an early version of the system was in human use at some sites in Europe. His task was to raise significant capital to get the product to a point where it was ready for the large scale pivotal trials that would take the company to FDA approval for both above- and below-the-knee applications.
A $20 million Series C round in April 2018, with major participants NEA (New Enterprise Associates), H.I.G. BioVentures, and Quaker Partners, helped advance a commercial version of the product through pivotal clinical trials in the above-the-knee indication. On the basis of TOBA II, the first peripheral vascular study in which 100% of patients had arterial dissections, the FDA granted Intact Vascular a PMA approval in April 2019.
Conducted at 33 clinical sites in the US and Europe, TOBA (Tack Optimized Balloon Angioplasty) II enrolled 213 patients with post-angioplasty dissections, 69.4% of them classified as severe. Operators used either plain angioplasty balloons or the Lutonix drug-coated balloon from the Bard Peripheral Vascular division of Becton Dickinson & Co. The study met both primary and secondary endpoints, demonstrating, at one year, complete resolution of the dissections in 92.1% of patients, a vessel patency rate of 79.3%, 86.5% freedom from clinically-driven reinterventions, and a low (0.5%) bailout stent rate.
That was the turning point for Intact Vascular, says Shook, the moment when they knew for sure that they had a valuable product. “That was a big day for us, when we saw those one-year results. We felt very confident at that point that we would get PMA approval based on those data,” he says.
In response to feedback from the company’s clinical collaborators, Intact Vascular took a different approach when designing TOBA III, a European post-CE mark study. The study enrolled 201 patients, a subset of them (32 patients) with long lesions (>150mm and≤250mm). This time, operators used Tack plus the IN.PACT Admiral, the market-leading DCB from Medtronic plc.
One-year results presented at the Transcatheter Cardiovascular Meeting in October 2019 were even more stunning. The therapy achieved 97.7% dissection resolution, 95% patency, 97.5% freedom from clinically-driven reinterventions, and a low (0.6%) stent bailout rate at one year. According to observational data, the patients with long lesions experienced 98.8% complete dissection resolution, 89.3% vessel patency, 96.8% freedom from clinically-driven revascularization, and a 0% bailout stent rate.
Expanding the Patient Population
Shook describes Intact Vascular’s market as one million angioplasties in the leg each year, a patient population that breaks down into two groups of disease; above-the-knee and below-the-knee. The former is the largest market in terms of procedure volumes, but in the latter, the Tack Endovascular System shines particularly brightly because it can change the lives of very sick patients with critical limb ischemia who have a very poor prognosis if blood flow to their lower limb is not restored. Patients with CLI face amputation rates as high as 40% at six months, and mortality rates of 20% to 25% within a year of diagnosis. (See “New Interventions for Critical Limb Ischemia,” MedTech Strategist, November 27, 2017.)
 As noted, at the recent VIVA meeting, six months results were presented on TOBA II BTK, Intact’s prospective, single arm clinical study for patients with CLI due to arterial disease below-the knee. At 41 sites in the US, Europe, and New Zealand, 233 patients with disease in themid/distal popliteal, tibial and/peroneal arteries were treated using standard balloon angioplasty followed by Tack. The participants were particularly challenging: 65.7% suffered from diabetes, at baseline, 83.7% had a Rutherford classification (a system for staging peripheral vascular disease) of 4 or 5 (anything above a 3 is serious), and 47.6% had chronic total occlusions.
As noted, at the recent VIVA meeting, six months results were presented on TOBA II BTK, Intact’s prospective, single arm clinical study for patients with CLI due to arterial disease below-the knee. At 41 sites in the US, Europe, and New Zealand, 233 patients with disease in themid/distal popliteal, tibial and/peroneal arteries were treated using standard balloon angioplasty followed by Tack. The participants were particularly challenging: 65.7% suffered from diabetes, at baseline, 83.7% had a Rutherford classification (a system for staging peripheral vascular disease) of 4 or 5 (anything above a 3 is serious), and 47.6% had chronic total occlusions.
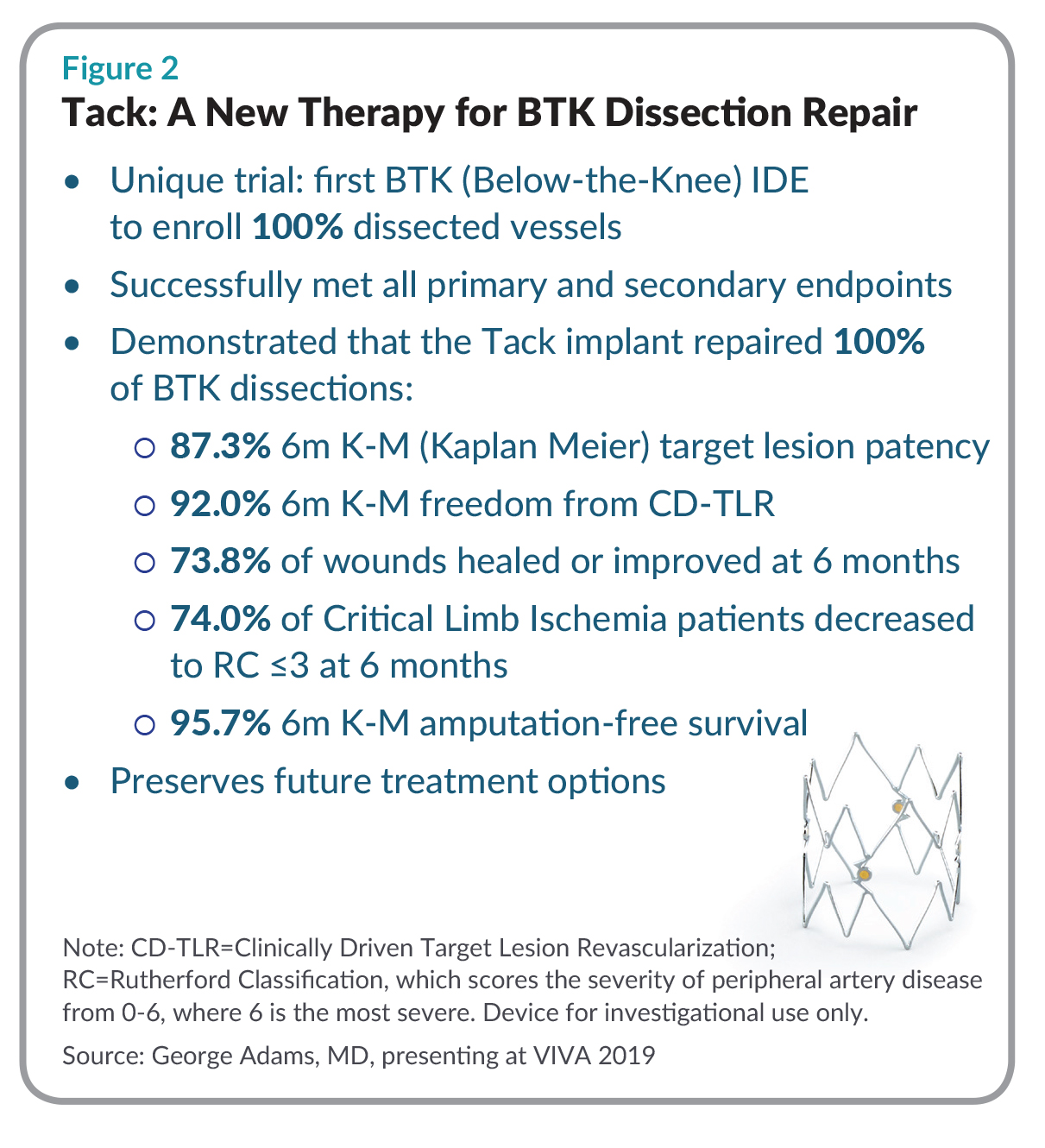
At six months, the Tack implants resolved 100% of the dissections (a total of 341), and 73.8% of leg wounds healed or improved. Most of the patients (95.7%) experienced amputation-free survival, 87.3% exhibited target lesion patency and a significant improvement in the toe brachial index (a measure of blood flow to the toes). The majority (92%) did not need a clinically driven reintervention (see Figure 2).
TOBA II BTK “has succeeded beyond our wildest expectations,” says Shook. The study puts Intact Vascular in a good position, since there are no implants approved for treating BTK disease, whereas there are probably as many as 10 stents approved for above the knee. “Tack is technically very well suited to treat tibial arteries, which are very small in comparison to the superficial femoral artery. Tack employs minimal metal. And you can see from our data that minimal metal works very well in the small, tibial arteries,” says Shook.
Intact Vascular has the opportunity not only to grow the BTK market when used with conventional angioplasty, but to enable many new technologies just entering the marketand on the horizon, among them, the intravascular lithotripsy catheter of Shockwave Medical Inc. for treating calcified lesions below the knee, which was just launched commercially, or perhaps a product like the Temporary Spur System of Reflow Medical Inc., in clinical studies outside the US, which is designed to treat BTK disease without leaving anything behind.
BTK disease has become a prime target for innovation. The Eluvia paclitaxel-eluting stent of Boston Scientific Corp., for example, was the first device for critical limb ischemia below the knee to be recognized by the FDA as a Breakthrough device, and is currently in pivotal clinical trials. (It must be noted, however, that although Eluvia uses the lowest therapeutic dose of paclitaxel, that drug has become controversial after a meta-analysis of clinical trials by Konstantinos Katsanos et al suggested that paclitaxel-eluting balloons and stents were associated with a long-term increased risk of death. See “Data debate: Paclitaxel Device Meeting Shows Rift in Regard for Real-World Evidence,” MTS Market Pathways, July 2019.)
In current applications, Shook says the company has polled users about what they would have done in a given circumstance, had they not had a Tack implant. “So far, we’ve learned that roughly 60% of the time they would have done nothing, because they would have been concerned about putting a stent in that particular patient.” In 40% of the cases, they said they would have used a stent, according to the company’s polling. “So we are taking stent share in 40% of the cases, but in 60% of the cases, we are actually expanding the market for an implantable device.”
The experience of interventional cardiologist S. Jay Mathews, MD, of Bradenton Cardiology Center in Bradenton, FL confirms those findings. Dr. Mathews says he’s treated more than 100 patients with different types of lesions in different locations since Tack became commercially available six months ago.“Before when I would see a dissection, the flow might look good, but I wasn’t happy with it, and I wouldn’t want to stent, so I’d say ‘let’s just hope it stays open.’” Now, it’s a routine finishing step. “We have placed our drug, we have done all this work, it’s a spot intervention with Tack, and we’re done.” Before Tack, he says, “It was a crap shoot; you had a dissection, you didn’t know how bad it was, and patients would come back—sometimes acutely, sometimes later. Now we can improve outcomes, improve patency, and minimize reinterventions.”
Just Right
“Intact developed the perfect ‘Goldilocks’ solution and it speaks to an unmet need in a significant percentage of interventions today,” says Justin Klein, MD, whose former firm NEA was an early investor in Intact Vascular. Klein has continued to support the company as a managing partner at Vensana Capital, which led the company’s $25 million financing round in May 2019. (Vensana is also an investor in Intact Vascular’s venous device spin-out, Vesper Medical Inc. See “Sibling Companies: A Model for Start-Up Efficiency?” MedTech Strategist, November 21, 2019.)
No other company had identified this opportunity, says Klein, believing the market to be well served by angioplasty balloons, atherectomy, and stents. “What wasn’t obvious was that there was a challenging clinical context in which there was no perfect solution for a significant number of cases,” he says.
It can be difficult for venture-capital backed companies to find those kinds of development opportunities in relatively mature categories in which there are at least a half dozen well-entrenched incumbents, Klein says. “It can be one of the more challenging business strategies to execute upon and get to an exit.” But Intact Vascular appears to be on the road to success.
No other company had identified this opportunity, says Klein, believing the market to be well served by angioplasty balloons, atherectomy, and stents.
At least some of Intact’s success can be credited to CEO Bruce Shook, who, over a 30-year career in the medical device industry, has led several companies breaking new ground. He was a co-founder and president ofNeuronetics, which, now publicly-traded, makes a non-invasive brain stimulation therapy for depression. He co-founded and led Neuron Therapeutics, which was developing a combination device/drug product for the treatment of certain CNS disorders, and earlier, as president ofAbiomed, he was instrumental in bringing the first ventricular assist device to the US market. He says he’s learned some valuable lessons.
“As an early-stage company, a pre-commercial company, you have to understand what will create the most value, and I have always believed that strong clinical evidence is a strong value creator. You have to make the investment in time and money to do robust clinical trials and prove that the technology really does work as advertised,” Shook says. That’s especially important for a company like Intact Vascular, which is the only company in its space. While that has allowed it to create valuable intellectual property, it comes with a high degree of skepticism.
It takes years, Shook says, and it is always tempting to shortcut that process. “But if you want to build a company with lasting value, it has to rest on a foundation of very solid clinical data. We have certainly done that at Intact; we have run five trials in total.” Admittedly, on $88 million in funding over eight years, the company has spent a lot of time and money doing so, but, says Shook, “now we are at the point where it is paying big dividends.”
