
ARTICLE SUMMARY:
With osteoarthritis a growing and under-treated public health problem, orthopedic surgeon Connie Chu’s group at Stanford is at the forefront of changing perceptions of the disease process, which has implications for orthopedics companies' strategies in one of their core therapeutic areas.
Constance R. Chu, MD, is leading the charge towards introducing new clinical treatments to prevent or delay the development of osteoarthritis.
As professor and vice chair of research in the Department of Orthopedic Surgery at Stanford University, she is pioneering multi-disciplinary approaches using advances in biologics, mechanics, and imaging towards this end.
The need is urgent:arthritis is the most common cause of disability in the US, with an estimated 54 million people suffering from clinically evident disease, according to the Centers for Disease Control and Prevention. OA, characterized by progressive damage to cartilage and other joint tissues, is by far the most common type of arthritis and the third most rapidly rising cause of disability (behind diabetes and dementia); some well-established databases show nearly 20% prevalence of OA in adults older than 45 years, according to the American Academy of Orthopedic Surgeons (AAOS; see Figure 1). Despite extensive research, no treatments effectively prevent or reverse OA. Although much attention has been devoted to identifying pharmaceutical and surgical therapies for early intervention, so far none of these are making much progress toward disease modification or prevention. Consequently, researchers say, current clinical care focuses on palliation. 
The AAOS is working to shift that paradigm, but the mechanisms and biology responsible for cartilage breakdown that lead to OA are only partially understood. Preclinical research has shown that there is a role for acute a nd sustained anti-inflammatory treatment in the prevention of OA. Furthermore, gene therapy approaches may offer an effective means for sustaining intra articular delivery of bioactive agents to restore joint homeostasis. (See “Farshid Guilak is Betting that 3D Biofabrics, Smart Cells and Drug-Device Combinations Can Fight Osteoarthritis,” MedTech Strategist, April 3, 2019.) But much work remains, and the findings have yet to advance to the clinic. Chu’s team is exploring these and other treatment strategies through a $10-million, four-year, peer-reviewed grant awarded to her by the US Department of Defense.
One route to greater understanding of OA disease progression involves better detection of what Chu has termed pre-osteoarthritis, which is characterized by identifying signs of increasing OA risk prior to development of the disease. Research groups are studying post-traumatic OA patients (PTOA), who are expedient subjects for this line of inquiry because they are at high risk of premature OA. Chu’s longitudinal studies differentiating young athletes who have had anterior cruciate ligament (ACL) ruptures into high risk and lower risk categories have yielded many insights into early disease progression. While her work is centered on basic and translational science, its ramifications are not lost on the commercial world. (See “How Zimmer Biomet’s Approach to OA is Shifting,” this issue.)
ACL tears—which are common i n teenage and young adult athletes—age the knee by up to 30 years. While ACL reconstruction surgery is effective in stabilizing the knee, it has not been shown to decrease the incidence of premature OA. Researchers are divided on whether new surgical techniques and anatomic reconstruction have reduced some of the OA risk in these patients. The hope is that identifying ACL patients at high risk of OA will enable them to take preventive measures such as maintaining fitness, avoiding certain activities, and losing weight.
The lack of advanced detection tools necessary to study the precise effectiveness of treatments on early disease progression has been a critical gap in the field, says Chu. Traditional diagnostic and monitoring approaches fall short; radiographic imaging is useful at more advanced stages of disease, but not for early, asymptomatic detection, and while the capacity for MRI to follow articular cartilage component changes is improving, it still falls far short of ideal. Newer technologies such as T1ρ (rho) and T2 imaging measure matrix and collagen integrity by looking at a series of signal decays over time. However, the ability to evaluate the dense, connective tissues for disease in the deep layers of articular cartilage requires special sequences that permit capturing ultrashort echo times (UTE).
Through a $4 million R01 grant from the NIH spanning more than a decade, Chu and her teamdeveloped non-invasive MRI UTE-T2* (Magnetic Resonance Imaging, Ultrashort Echo Time T2*) mapping for diagnosis of pre-osteoarthritis. It produces color maps that show variations in the deep layers of cartilage that are undetected by regular MRI (see Figure 2).There has been a long-standing debate regarding whether OA begins in the bone or the cartilage. The earliest changes likely occur in both tissues at the cartilage-bone junction, but we have not been able to visualize these changes until now.
“The MRI UTE-T2*, which allows me to see ‘pre-osteoarthritis’ has been the missing component to progressing preventive treatment strategies from the laboratory into clinical trials,” Chu says. Moving forward, she and her team will employ this imaging technique in her DOD-funded clinical trials studying biologics, gene therapy, and gait retraining to treat joints early after injury to help thwart OA.
Chu’s advanced imaging studies also are contributing to the identification of biological blood-based biomarkers suitable for characterization of a pre-OA joint. These markers could be another foundation for development of effective early prevention and treatment strategies for OA, similar to how testing cholesterol levels is now used as a standard potential indicator for heart disease and high blood sugar for diabetes, she believes.
Poor test results could alert patients and providers to the need for early intervention. “In the case of pre-osteoarthritis, whether it’s the physical therapy, medication, or biologics, we can now use early detection technologies to start to see if these interventions make a difference in reducing OA risk,” she says.
Chu has earned more than 30 honors for her work on early diagnosi 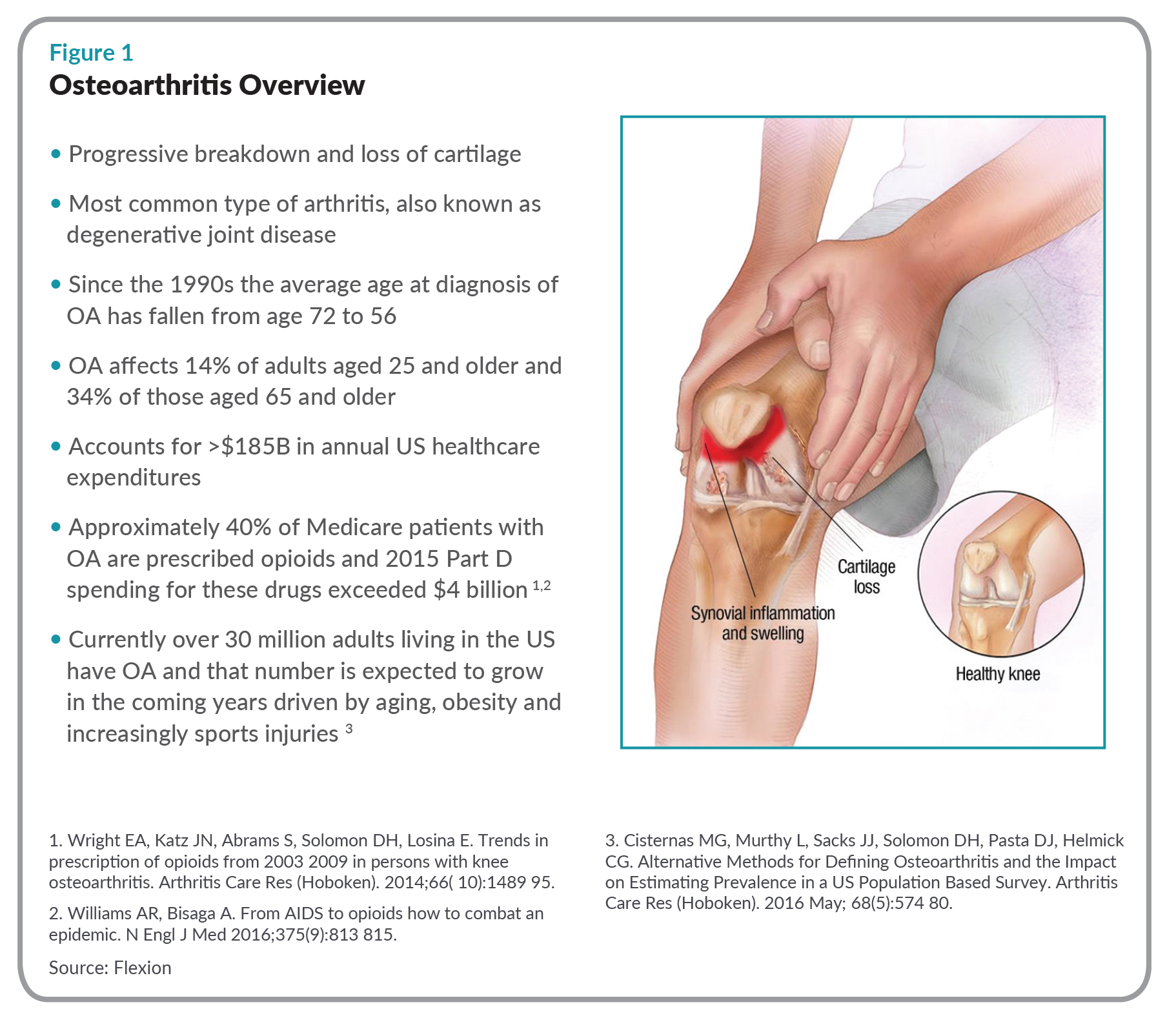 s and staging of joint and cartilage injury. In March , she received the prestigious Kappa Delta Award, given at the AAOS annual meeting in recognition of a large body of work that advances the field of orthopedic surgery. The award manuscriptcovers 42 studies over 10 years. “What we accomplished was to define an entity of pre-osteoarthritis which now opens the door to identifying people at risk for OA before they develop the disease,” Chu says. “The clinical trials underway aim to see if we can reduce that risk with our interventions and thereby prevent or delay OA onset.”
s and staging of joint and cartilage injury. In March , she received the prestigious Kappa Delta Award, given at the AAOS annual meeting in recognition of a large body of work that advances the field of orthopedic surgery. The award manuscriptcovers 42 studies over 10 years. “What we accomplished was to define an entity of pre-osteoarthritis which now opens the door to identifying people at risk for OA before they develop the disease,” Chu says. “The clinical trials underway aim to see if we can reduce that risk with our interventions and thereby prevent or delay OA onset.”
MedTech Strategist interviewed Chu earlier this year at the AAOS annual meeting on her ground-breaking work.
MedTech Strategist: How did your research evolve?
Constance Chu: I started working to regenerate articular cartilage using stem cells and biodegradable scaffolds shortly after my internship and thought that cartilage tissue engineering would solve the OA problem in a few years. I quickly learned that, while it was easy to grow cartilage tissues in the laboratory, regenerating damaged human cartilage was a bigger challenge. By the time I finished my residency, I realized OA was not so much a cartilage problem but one of the most common, debilitating, and challenging problems in orthopedic surgery.
As an attending surgeon, I started to see the whole spectrum of joint diseases in my patients. I became particularly interested in articular cartilage ligament injuries because my practice included both young patients coming in with ACL tears and slightly older patients in their 30s and 40s with advanced osteoarthritis who had torn their ACL 10-20 years previously. The patients coming in with new ACL tears were typically active and had pretty normal joints before the injury, while those coming in having torn their ACL years ago were unable to fully participate in work, sports, or life, and had advanced OA . This highlighted to me that something happens after tearing the ACL to fast track the degenerative process so that the risk of osteoarthritis goes sky high, to the point where about half of patients—and these are young people—already have osteoarthritis 10-15 years later. Trying to improve what we can do for my patients has led me to focus on post-traumatic OA.
So they could be injured in their 20s, and by the time they're in their late 30s, early 40s, they have osteoarthritis?
Yes. Most of the ACL tears occur in teenagers, so they could be in their late 20s and early 30s and essentially have knees that already limit them, with some even coming in to ask about a total knee replacement. I started searching biologically, mechanically, and structurally for answers, and it all pointed toward early intervention before symptoms of OA even develop.
However, it is hard to motivate change or to justify interventions that may be difficult or expensive when there doesn’t seem to be a problem. Nevertheless, I thought that if people could see that something is wrong, that it would really register. This began my search for a means to see and measure changes that reflect a higher risk of developing osteoarthritis before the disease develops.
Is high risk of re-injury inevitable if you get an ACL injury?
Yes, ACL-injured patients have a higher risk of re-injury to both the injured knee and the contralateral knee. However, the greatest long-term risk to the knee is the development of PTOA [ post-traumatic osteoarthritis] and premature OA. If you truly want to prevent PTOA, you need to prevent joint injuries. But as orthopedic surgeons, we know that there are situations whether through sports, work, or being in the wrong place at the wrong time where people will continue to get injured. And once someone is injured, we know the risk is there. Thus, it becomes important to identify and monitor high-risk individuals, and to develop effective early intervention strategies.
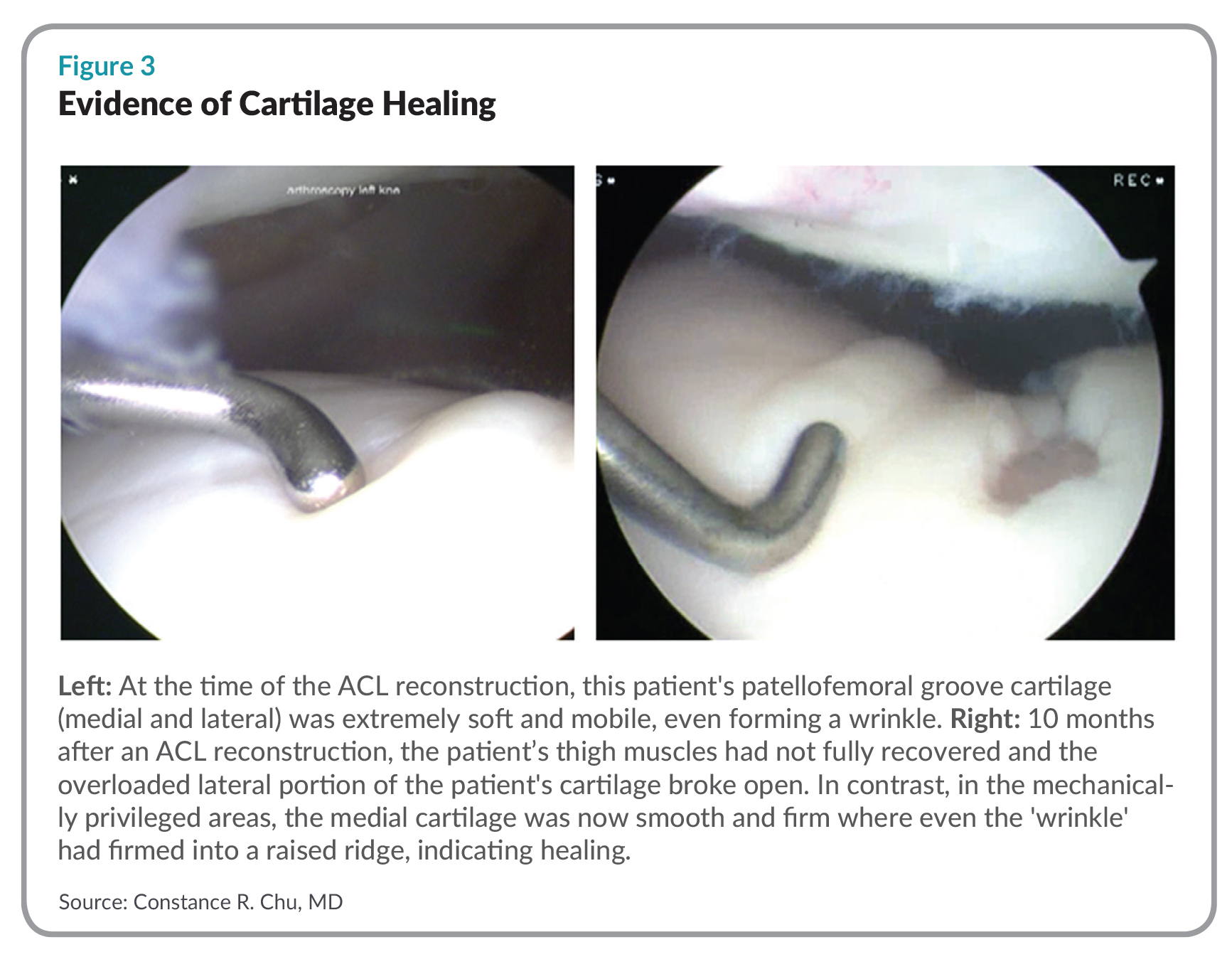
My research shows that if the surface of the cartilage is still intact, the cartilage can potentially heal. [She points to an image of a young patient with an ACL rupture] This patient, for 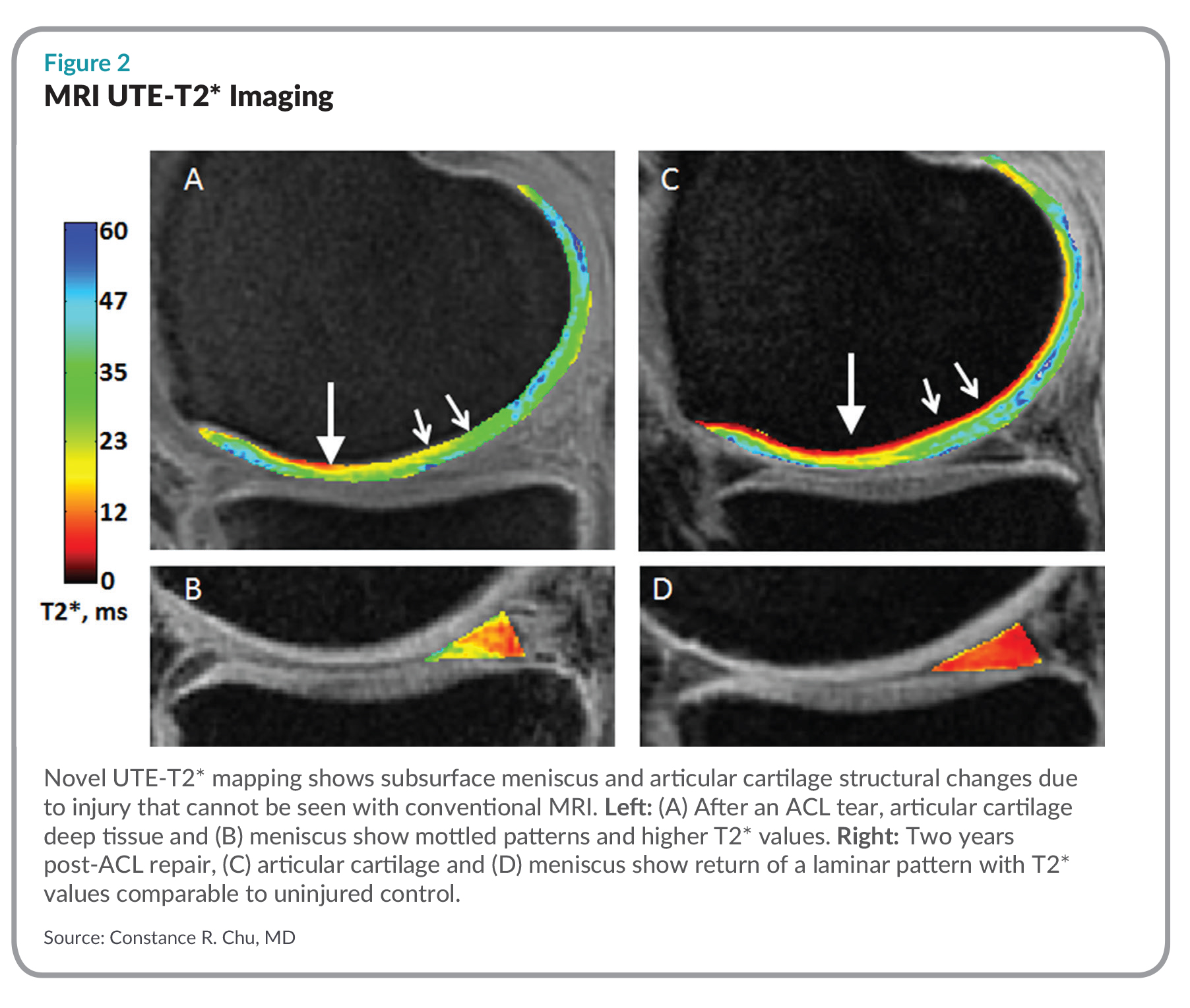 example, at surgery, had very soft cartilage with a surface that was still intact. Part of it healed and part of it broke open five months after surgery (see Figure 3). This occurred because the patient didn’t recover sufficient strength to the inside of the thigh. This meant that whenever she bent and straightened her knee, the kneecap ran over only the outer half of the kneecap groove and overloaded it. The overloaded half broke open. The other half ended up healing.
example, at surgery, had very soft cartilage with a surface that was still intact. Part of it healed and part of it broke open five months after surgery (see Figure 3). This occurred because the patient didn’t recover sufficient strength to the inside of the thigh. This meant that whenever she bent and straightened her knee, the kneecap ran over only the outer half of the kneecap groove and overloaded it. The overloaded half broke open. The other half ended up healing.
This did not occur in isolation. The cartilage that broke open was already weakened. I could tell when I examined it during her ACL surgery. The cartilage surface was wrinkled but still intact. When I lightly pushed on it, however, the cartilage indented deeply and moved in a fluid fashion, meaning that it was abnormally soft down to the bone.
What caused the softness and how was the damaged cartilage different?
Possible causes include bleeding into the joint from the ACL tear leading to persistent inflammation which compromises the cartilage tissue. The extreme softening meant that this cartilage was severely damaged and at high risk of breaking open.
“I believe you can build cartilage up if the surface has not broken down. But, I don’t have the answer to whether high-risk parties will always be extra vulnerable to OA.”
It’s just as important to show that she healed as that she didn’t heal.
Yes! This patient taught me so much because half of the cartilage healed. The difference between the part of her cartilage that healed and the part that did not was because her thigh muscle imbalance resulted in the kneecap overloading the cartilage that broke open.
To what extent can that vulnerability be addressed by preventive treatment such as physical therapy?
Sustained physical therapy to improve form, core strength, and balance muscle activity likely would have reduced loading to what her cartilage could handle and helped prevent the surface from rupturing. As with many people, it was difficult for her to obtain adequate physical therapy. Some of the reasons included a need to return to work, the expense, and the seeming recovery of the knee itself, which appeared to have recovered well enough within a few weeks of surgery to where the additional time and cost did not seem justified.
The absence of symptoms is a big reason OA is so hard treat—because we don’t know the cartilage is damaged. If you cut your skin or you bruise your thigh, it hurts, so you don’t use it as much until it heals. With the cartilage, it doesn’t have nerves, so it doesn’t feel pain, and there are no symptoms until it breaks open and you still don’t feel any pain. Over a long time, it wears away and then you have pain when bone rubs against bone or the synovium gets inflamed, and it’s too late to reverse the process.
This is why I worked so hard to identify cartilage at a vulnerable stage before it breaks open. Now we can alert patients and we can develop and institute new treatments. We can also evaluate new treatments to see if the cartilage stabilizes or heals.
Your work on more precise imaging technology won the Kappa Award at AAOS this year. How does the new imaging modality work and what differentiates it from standard work ups?
 On a regular clinical MRI of a joint surface cartilage in two patients, both patients seem to have normal cartilage. Our UTE-T2* maps of the same patients, however, show the cartilage and menisci look very different. We were able to demonstrate in other studies that the UTE-T2* imaging of patients two years after ACL surgery correlate with mechanical markers of OA risk, biological markers, and patient reported outcomes. This meant that the damage we saw on the UTE-T2* maps is clinically meaningful. Best of all, we showed that the UTE-T2* changes reversed themselves over time in some patients, suggestive of healing. This means that MRI UTE-T2* mapping detects joint damage early enough to where the disease course can be modified or even prevented.
On a regular clinical MRI of a joint surface cartilage in two patients, both patients seem to have normal cartilage. Our UTE-T2* maps of the same patients, however, show the cartilage and menisci look very different. We were able to demonstrate in other studies that the UTE-T2* imaging of patients two years after ACL surgery correlate with mechanical markers of OA risk, biological markers, and patient reported outcomes. This meant that the damage we saw on the UTE-T2* maps is clinically meaningful. Best of all, we showed that the UTE-T2* changes reversed themselves over time in some patients, suggestive of healing. This means that MRI UTE-T2* mapping detects joint damage early enough to where the disease course can be modified or even prevented.
This what we won the award for, because now we can identify ‘pre-osteoarthritis’—that the risk for OA is rising before irreversible changes and OA itself develops. Now we can start to answer the questions that everybody is asking about whether a specific new therapy reverses or reduces changes of “pre-OA”. Once we find treatments that can prevent or reverse ‘pre-OA’, we can prevent OA.
And is this tacking on additional software and instrumentation to a regular MRI?
This is research software that runs on standard MRI equipment. It allows us to acquire the image and then we have different software that we use to process the image to generate the maps. We do have to obtain several images at different echo times to bring out this detail.
Once you have weakened cartilage, can you rebuild it so that it regains its strength or the only thing you can do is prevent further deterioration? Will the injured parties always remain at high risk of OA?
I believe you can build cartilage up if the surface has not broken down. But, I don’t have the answer to whether high-risk parties will always be extra vulnerable to OA. Here’s what I think, however. If your cartilage is weakened and you overload it you increase your risk. But there are training techniques, which are not standard right now, to improve how people use their joints and can very easily be incorporated into a physical therapy regimen.
Are you incorporating any of this into your practice?
Slowly, because as a scientist, you're always looking for additional proof. But I think if you show somebody a map of their injured knee and it looks different from their uninjured knee, they're going to suspect something is wrong and ask, ‘Well, what can you do about it?’ But the hesitation is, what if this imaging technology is too sensitive? That’s why longer-term studies are needed, to definitely show that this technology does, in fact, predict the risk of osteoarthritis. Our studies currently do not go out that far.
Do you need a specialist to read the imaging technology or can it be done in a community hospital setting? Do you eventually envision that it can be done on a broad scale?
Eventually, it most likely can be done in a community setting. We use existing equipment, such as scanners that are widely used clinically. The software is a little bit different to acquire the scans. The biggest challenge is the image processing which now takes highly skilled people quite a bit of time to do. There are new developments in automating some of the most time-consuming parts and in artificial intelligence that can help bring this into mainstream medicine for preventive care.
