
ARTICLE SUMMARY:
Cardiac Dimensions is the rare start-up from the first generation of percutaneous mitral valves that’s still standing, but in the 20 plus years since its founding, the market has moved toward the company. Only one more hurdle stands between it and an expanded patient population that, upon FDA clearance, only its device can serve.
Transcatheter aortic valves proved to be so clinically and financially successful that it was only natural for medical device developers to try to replicate that model in mitral valves. After aortic-valve leader Edwards Lifesciences acquired minimally invasive mitral valve replacement company CardiAQ Valve Technologies in 2015, a veritable feeding frenzy ensued, with further mitral valve acquisitions made by Edwards, Abbott Laboratories, Medtronic, and Boston Scientific. (See “Transcatheter Mitral Devices: The Dam Finally Bursts with a Flood of Deals,” MedTech Strategist, August 31, 2015.)
These mitral valve start-ups were positioning themselves to serve a large patient population suffering from functional mitral regurgitation (FMR), a type of mitral regurgitation that tends to arise from left ventricular volume overload and remodeling (due to damage caused by myocardial infarction or heart failure, for example).
Approximately 50% of people who suffer a myocardial infarction and about half of heart failure patients develop FMR. When one considers that about five million people in the US (more than 20 million worldwide) suffer from heart failure, the potential market for FMR treatment is enormous. The overall prevalence of the condition in those over the age of 75 is estimated at 10%.
Without treatment, at three years, patients with FMR face survival rates of about 51%, and their probability of surviving three years without experiencing hospitalizations for heart failure is only about 20% (according to an article published in 2023 in the European Heart Journal, by Teo et al).
But despite the abovementioned frenzied IP land grab of 2015, only three companies have minimally invasive mitral valve repair or replacement products on the market today, two of them giant medical device companies and leaders in transcatheter heart valves. In the US, Abbott offers MitraClip (valve repair), and Edwards sells PASCAL (valve repair) as well as the Mitris Resilia (for mitral valve replacement). Cardiac Dimensions, the lone small company in the top three, has been selling the percutaneous Carillon Mitral Contour System for valve repair in Europe since 2011. (A fourth product, NeoChord, which has had the CE mark since 2013, specifically repairs the chordae tendineae in cases of mitral valve prolapse.) As for the dozens of other companies that set out on the journey, several prematurely acquired for their IP, many have fallen by the wayside due to their products’ insufficient safety and or efficacy.
Lone Survivor
A member of the first generation of percutaneous mitral valves, Cardiac Dimensions, founded in 2000, has steadfastly persisted for more than two decades, and as the sector has evolved, the market has moved in the company’s direction, as clinicians now prefer repair over replacement when possible, percutaneous transcatheter delivery rather than apical access through the chest, and, over time, have come to recognize the role FMR plays in heart failure. FMR and heart failure exacerbate each other, and mitral dysfunction should be treated to reverse heart failure’s negative trends.
Today, Cardiac Dimensions finds itself with a product backed by efficacy data from rigorous clinical trials, and which is unique in offering two desired effects: acute FMR reduction to help patients feel better in the near-term, plus longer-term positive remodeling of the left ventricle to address the root cause of the FMR, for improved survival, reduced heart failure hospitalizations, and enhanced quality of life.
The fact that the small company has survived for 20-plus years in a market dominated by large strategics is testament to the differentiating advantages its Carillon device offers. It meets the market’s desire for a product that’s easy to use and very safe, and such an enhanced level of safety is why the FDA granted the company, in its US pivotal EMPOWER trial, the ability to include patients with lower grades of MR than the other approved devices.
While longevity for a single-product start-up can be challenging in terms of continually grabbing headlines for the kinds of incremental advancements possible on a start-up’s budget, Cardiac Dimensions now stands on the brink of an opportunity to expand the transcatheter mitral valve market and treat patients no other company can.
A Safer Solution
The Carillon Mitral Contour System deals with a common cause of mitral regurgitation: the failure of the native leaflets to coapt, thus leading to regurgitation. The leaflets themselves might be functional and healthy but dilation of the heart, which enlarges the annulus of the mitral valve, prevents them from coming together. “The door frame becomes too big for the doors,” says Rick Wypych, who joined the company as president and CEO in 2003.
The Carillon device has distal and proximal anchors connected by a shaping ribbon that uses the heart’s venous anatomy to cinch the mitral annulus (see Figure 1). “We are cinching the door frame to fit the doors,” Wypych says, noting that in contrast, MitraClip “pulls the doors together, without fixing the underlying problem of an enlarged annulus.”
If it seems that early on, this percutaneous take on annuloplasty was common among companies targeting mitral valve repair, Wypych points out, “We developed an immense amount of IP and locked those companies out. They had to be creative to get around the IP, and their devices were either difficult to use, didn’t yield efficacy, or were difficult for the patients to tolerate in terms of procedure time or blood transfusions.”
Wypych notes that there are many benefits to his company’s approach. The transcatheter device works in the coronary sinus, a vein on the outside of the heart that is slightly superior to the annulus of the valve, accessed through the right jugular vein. The catheter travels as far distally as possible, then the operator locks the distal anchor. The operator pulls tension to cinch the annulus and deploys the proximal anchor to lock the device in place.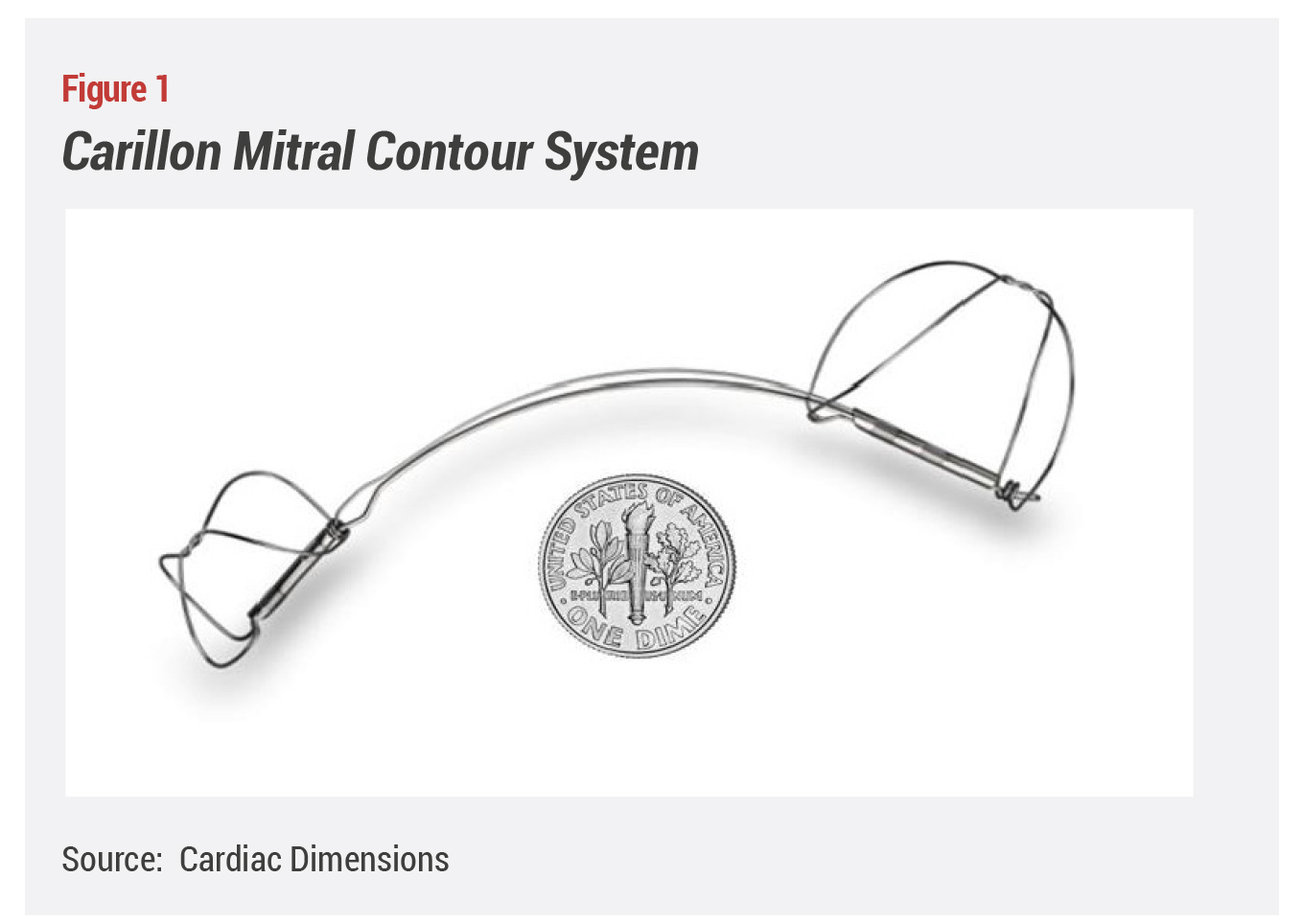
Cardiologist Klaus Witte, MD, chief of device therapy at the Uniklinik in Aachen, Germany, has implanted 30 Carillon devices and proctored many more procedures. He confirms that the procedure is safe, simple, and fast. “It is an entirely venous approach. You are not putting anything into systemic circulation, which eliminates the risk of stroke. You don’t need to cross into systemic circulation as you do with MitraClip or other mitral procedures.”
Because the implant is delivered via the venous system, “You can do it in old people and multi-morbid patients. It doesn’t require anesthesia and an anesthetist,” says Witte. “You can do it with local sedation and a little bit of additional sedation if the patient is anxious.” The mode of delivery of the Carillon also eliminates other procedural steps, Witte adds. “You don’t need to place a transesophageal echo probe down the patient’s throat, so from this perspective, it is easier to do and could be done in a day surgery,” although he notes that from a reimbursement standpoint an overnight stay might be required. “The procedure itself takes 30-60 minutes, if you know what you are doing,” he says.
The chief safety issue of the procedure results from the proximity of the circumflex coronary artery and the coronary sinus vein at the back of the heart. In Witte’s experience, in about 5-10% of patients, when the operator tensions the device, it presses on the circumflex artery with the potential to obstruct flow, “which is rarely a problem because you can release the tension a bit to ease pressure on the artery.”
Wypych explains that the operator can assess the safety of the implant (that it doesn’t impinge or obstruct the flow in the circumflex coronary artery, for example) and the degree of MR reduction, prior to the release of the implant. If satisfied, they decouple the device. “If we don’t like what we see, for example, if we think we can get a better result with a different size of the device or placement, we recapture the device, and simply reverse the procedure. That significantly decreases the risk of a patient ending up with a metal implant that doesn’t benefit their life.”
We have never had to explant a device and we see very few safety events related to the device or procedure. We’re proud that we have both a device and procedure that are extremely safe.
Once the device is decoupled, it endothelializes with the vein within 6-8 weeks. “We have never had to explant a device,” Wypych notes, “and we see very few safety events related to the device or procedure. We’re proud that we have both a device and procedure that are extremely safe.”
Finally, Carillon is easy to deliver. “It typically takes 50 cases for physicians to get certified using clips; it only takes three for Carillon.” Wypych adds, “The first case we did at a new site yesterday took only 14 minutes, from start to finish. Other therapies can take hours in the cath lab.”
As noted, implanting Carillon doesn’t require general anesthesia, multiple physicians, or the same level of imaging as clips, and patients don’t need to stay in the ICU as they do after procedures with other devices. “All of these things might limit the use of other therapies to very large institutions that have surgical backup and other advanced care. But if you can implant a stent in your lab, you can put in Carillon. Those are some of the reasons why we consider our device safe, simple, and effective,” says Wypych.
Taking No Shortcuts
From the outset, Cardiac Dimensions faced the challenges that all medical device start-ups face when competing with large, deep-pocketed multinational corporations able to outspend them. Wypych says they knew they could only succeed with a superior product backed by a high level of evidence. The company has taken no shortcuts. “Sham controlled blinded trials are the absolute pinnacle,” states Wypych.
The clinical effectiveness of Carillon has been demonstrated in four studies, the most recent of which, REDUCE FMR, was the first double-blinded, randomized, sham-controlled trial of a percutaneous heart valve therapy. In the study (which was published in November 2019 in JACC: Heart Failure), 120 patients with an FMR grade of 2+, 3+, or 4+ and on medical therapy were randomized 3-1 (treatment to control) to either Carillon or a sham procedure. Assessments were done at a core echocardiography laboratory at the Cleveland Clinic by clinicians blinded to the patients’ study allocation.
At 12 months, investigators found a median 22.4% decrease in MR in the treated group, versus 1.5% in the control arm. At one year, there was also evidence of reverse (positive) remodeling with significant decreases in the left ventricular volume, and patients in the treatment group had a greater improvement in six-minute walk distances. Finally, further analysis showed a 60% reduction in heart failure hospitalizations and death for treated patients. According to the study, treatment effects were even greater in patients with more severe grades of FMR. As a testament to the ease of use of the device, the REDUCE FMR authors point out that for the most part, the study was conducted at centers previously unfamiliar with Carillon.
To make sure the evidence was highly credible, “We were core-lab reviewed, adjudicated by CEC/DSMB [Clinical Event Committee/Data and Safety Monitoring Boards] and third-party monitored, by groups like Cleveland Clinic, Columbia, and Brigham and Women’s, so we have set a very high standard with regard to clinical data,” says Wypych.
Witte, who is lead author of the REDUCE FMR study, notes that it is the only sham-controlled study in this field. “The others have been open label and flawed as a result of the difficulty in blinding patients.” With REDUCE FMR, patients didn’t know whether or not they got the device. At the University of Leeds, where Witte is a consultant cardiologist, he says patients would wear headphones playing music and wear glasses so they couldn’t see or hear the procedures. All patients were punctured and cannulated. “It wasn’t until the device was measured that they were randomized to having one or not.” The ongoing EMPOWER US pivotal trial is blinded with equal rigor, Witte notes.
A Population Approach to Heart Failure
Witte says he became interested in Carillon as a heart failure cardiologist. “I mainly implant CRT [cardiac resynchronization therapies] in the coronary sinus. I don’t perform TAVI [transcatheter aortic valve implantation].” Of particular interest with respect to heart failure, studies of Carillon have clearly shown positive heart remodeling. “It probably struts the heart, so it not only reduces the mitral valve orifice, it also stops the heart from further dilation,” he suggests. Even in patients who haven’t experienced a significant reduction in MR following Carillon implantation, “It holds off further deterioration and that is something that concerns heart failure physicians. This works by helping the heart reshape itself or by preventing further adverse reshaping, and that’s why putting it in at an early stage is likely even more effective.” And, as noted, as heart dilation decreases, MR tends to decrease. In contrast, Witte says, “MitraClip actually treats the MR, but from all the data we’ve seen, it doesn’t actually treat the cause of MR, which is remodeling.”
Of particular interest with respect to heart failure, studies of Carillon have clearly shown positive heart remodeling. “It probably struts the heart, so it not only reduces the mitral valve orifice, it also stops the heart from further dilation.
That’s why the safety of Carillon presents a compelling opportunity to treat patients early enough to stave off heart failure. Says Witte, “This is the sort of device you can use on a population level. Say I have a patient who fits the bill for potentially adverse remodeling going forward, so I’m going to intervene early.” At the same time, since the patient is not yet in a high-risk group, “I don’t want to treat that patient with something high risk that’s going to take five hours to implant. I want a low-risk treatment.” On the other hand, he continues, “If you have something that is incredibly difficult to do, it will only be used in a small number of people. And if it is incredibly difficult to do, it better perform brilliantly, because the risks are so high.”
Wypych emphasizes that the right-heart approach preserves future therapy options, which strengthens the argument for early intervention. “If later you want to implant a MitraClip, an LVAD [left ventricular assist device], or a pacing lead, you can, because going through the coronary sinus as we do doesn’t preclude the use of these types of therapies later.”
In Europe, the company has created a real-world registry called CINCH. Data from patients treated commercially (i.e., all comers as opposed to carefully screened clinical trial participants) has been pooled from all the sites that have signed up. “In the commercial environments, clinicians will use your device at the extremes of your indication, so you might have very sick patients or extremely healthy patients not normally included in a clinical trial,” says Wypych. An analysis of the first 100-patient slice of the data, which was presented as a poster at the TCT [Transcatheter Cardiovascular Therapeutics] meeting in 2022 “was absolutely confirmatory of all of our studies, even slightly better than our clinical trial,” Wypych says.
Standing on the Brink
In Europe, Wypych says sales have doubled over the last couple of years and the company has been expanding into different geographies that are large markets with high reimbursement. “As a small company we need to be selective so we don’t spread ourselves too thin. We are rolling out in a measured way, looking for high-quality, repeatable sales at high-quality institutions.” Abroad, Carillon competes with clips. But it has a unique strategy for the US market.
The FDA clearances for both MitraClip and PASCAL specify the treatment of patients with mitral regurgitation grade III or above because of the risk profiles of the devices—they require a transseptal puncture and a patient stay in the ICU, as noted earlier. For Cardiac Dimensions’ US EMPOWER trial, the FDA has allowed the company to recruit patients at earlier stages of disease—grade I or above—because of the superior safety and ease of use of Carillon. Wypych notes that if one goes by the inclusion and exclusion criteria for the MitraClip pivotal study, “Our market could be up to five times larger than the existing clip market.”
In addition, the FDA granted the company a Category B designation, which allowed it to petition CMS for reimbursement of both the study device and all items related to the standard of care for data collection and follow-up during the trial. “So, we are actually selling the device during the US trial,” Wypych says. “We have a full DRG that is active, which we are billing against in our US pivotal study. They have granted us payment rights well in advance of what a company would typically see in any sector.”
This is great support for Carillon, which, Wypych emphasizes, “cuts hospitalizations by half. We have publications out to seven years that show 60% survival rates. We also reduce heart failure hospitalizations, and that’s where the cost to the system is. The reimbursement rates are high because we save much more than that by treating the patients.”
Cardiac Dimensions has begun recruiting for EMPOWER, a prospective, randomized, blinded clinical trial enrolling 300 subjects at 75 sites in the US, Canada, and Europe. Patients will be randomized 1:1 to the intervention or the sham. “To make sure the study goes well,” Wypych notes, “we have been hiring a significant team to oversee, enroll, and collaborate with the sites involved in this landmark trial.”
In January, the company raised a $35 million Series D round to support enrollment in EMPOWER as well as sales expansion in Europe. The recent financing was led by existing investor Horizon 3 Healthcare and an undisclosed strategic investor with the participation of existing investors Arboretum Ventures, Hostplus, EQT Life Sciences, Lumira Ventures, and MH Carnegie & Co. Over its 23 years in existence, Cardiac Dimensions has raised more than $200 million, “which is probably substantially less than you would expect. We are a thoughtful and frugal company, and we have been able to do a lot with little money,” Wypych says.
